2025 Proposed CMS Rule for the Medicare Physician Fee Schedule
2025 Proposed CMS Rule for the Medicare Physician Fee Schedule
In July, CMS published the Proposed Rule for the 2025 Medicare physician fee schedule. Overall, BSA Healthcare estimates that emergency medicine will undergo a 1% to 3% decrease in payments in 2025 compared to 2024 payments.
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
CMS estimates a 2025 conversion factor of $32.3562. Compared to the 2024 conversion factor of $33.2875, the 2024 conversion factor represents a 2.8% decrease. Like previous years when Congress passed one-time fixes to the SGR formula, Congress in 2023 passed a one-time 2.93% increase in the conversion factor. That 2.93% increase expires at the end of 2024. Because of suggested changes to the global-surgery packages, there is no budget neutrality decrease in the conversion factor for 2025. In fact, a small budget neutrality increase caused the projected 2.93% decrease to be slightly reduced. The final 2025 conversion factor will be published in November 2024. There is a possibility of late-year Congressional action to partially mitigate the CF decrease.
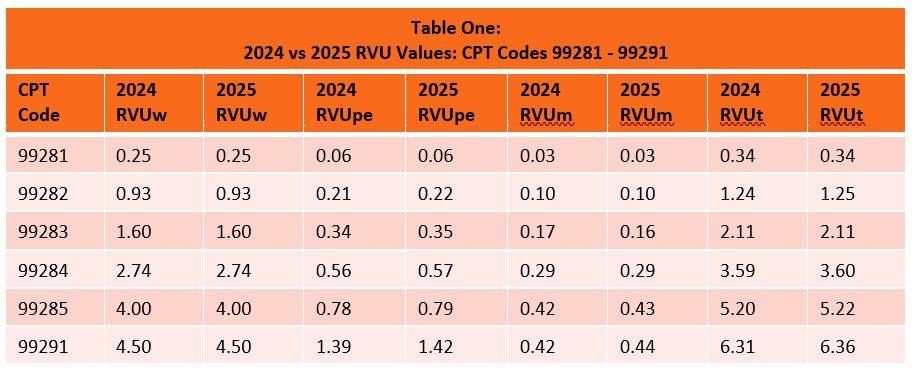
Relative Value Units for 2024
CMS has proposed minimal RVU changes for emergency service code practice expense and malpractice RVUs in 2025. Work RVUs remain unchanged for 2025. Overall, emergency service code RVUs are flat in the proposed rule.
Budget Neutrality Provisions Affecting the Conversion Factor
Because CMS is statutorily mandated to maintain budget neutrality when changes are made to the physician fee schedule, the 2021 RVU increases for office visit codes caused a reduction in the conversion factor for all CPT codes, including emergency services.
At the end of 2020, Congress mitigated the significant reduction in the 2021 conversion factor by adding a one-time increase of 3.75% to the conversion factor. At the end of 2021, Congress mitigated the significant reduction in the 2022 conversion factor by adding a one-time 3% increase to the conversion factor. At the end of 2022, Congress mitigated the significant reduction in the 2023 conversion factor by adding a 2.5% increase to the conversion factor in 2023 and 1.25% in 2024. The initiation of the G2211 code in 2024 caused another 2.1% reduction to the conversion factor. Congressional action to mitigate the impending 2025 2.8% reduction in the conversion factor is uncertain. BSA Healthcare feels that Congress will partially mitigate the 2.8% decrease in the conversion factor for 2025.
Pay-as-you-go budgetary 4% sequestration reductions are suspended through 2024; however, the ongoing 2% sequestration remains in effect. Most likely, although not assuredly, Congress will again suspend the 4% pay-as-you-go sequestration in 2025. In sum, emergency medicine is facing a potential 1% to 3% reduction in payments caused by the conversion factor decrease.
Budget Neutrality Purgatory
Medicare’s budget neutrality provision for Part B physician services stands in stark contrast to federal funding mechanisms for Part A (hospitals), Part C (Medicare Advantage), and Part D (prescription drugs). Funding for these other three Parts is based on inflationary or cost increases. Strikingly, commercial insurer Medicare Advantage Plans continue to receive between 5% to 8% funding increases despite many of these plans being under federal fraud investigation for billions of dollars of overpayments based on deceptive diagnostic coding. Only Congress can change Medicare funding formulas, so Congressional action is required to modify the Part B budget neutrality provision. Currently, legislation is being proposed to adjust the Part B formulation to include inflationary increases, but expeditious passage of such legislation remains unlikely.
Since 2020, the conversion factor has decreased by 9.25% from 36.0893 to 32.7442. At best, budget neutrality provisions lock in flat MPFS rates in the future before inflation. The potential for continued CF reductions exists every time a new code is added or RVUs are adjusted to favor certain physicians. Nothing will change unless Congress addresses the MPFS funding structure.
One remote possibility for enhanced funding for emergency services exists in the form of EMTALA-related funding for physicians who provide safety net services. The Emergency Medicine Practice Institute is financially backing an effort to develop an effective EMTALA narrative. Success is by no means guaranteed. It will take years and will require Congressional action.
Practice Expense RVU Input
CMS has historically relied on surveys performed by the American Medical Association (AMA) to determine the practice expense RVU for each CPT code. A recent survey was performed by the AMA, with closure of the survey instrument in April 2024. As in past surveys, response rates were anemic. There is a possibility that the AMA will reopen the survey. In the proposed rule CMS states that they are contracting with the RAND corporation to evaluate alternative methods for determining practice expense RVUs. No action is envisioned for 2025. Organized emergency medicine is hopeful that EMTALA related uncompensated or undercompensated care will be considered by CMS to be a valid practice expense.