2025 Final CMS Rule for the Medicare Physician Fee Schedule: CMS-1807-F
2025 Final CMS Rule for the Medicare Physician Fee Schedule: CMS-1807-F
In November, CMS published the final rule for the 2025 Medicare Physician Fee Schedule (MPFS).
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
CMS assigned a 2025 conversion factor of $32.3465, which is approximately 2.83% lower than the 2024 conversion factor of $33.2875. The primary cause for the conversion factor reduction was the expiration of the 2.93% one-year conversion factor increase passed by Congress for 2024.
Congressional action to mitigate the CF decrease with a 2.5% one-year increase for 2025 was meant to be included in a continuing resolution at the end of 2025. At the time of publication, we are awaiting the CMS release of the revised 2025 conversion factor.
Sequestration
The 2024 end-of-year Congressional legislation was meant to contain two important provisions affecting physician reimbursement. At the time of publication, we are awaiting official CMS notification of the following:
- The continuation of the 2% sequestration cut.
- Continued postponement of the 2023 pay/go 4% sequestration cut until 2026.
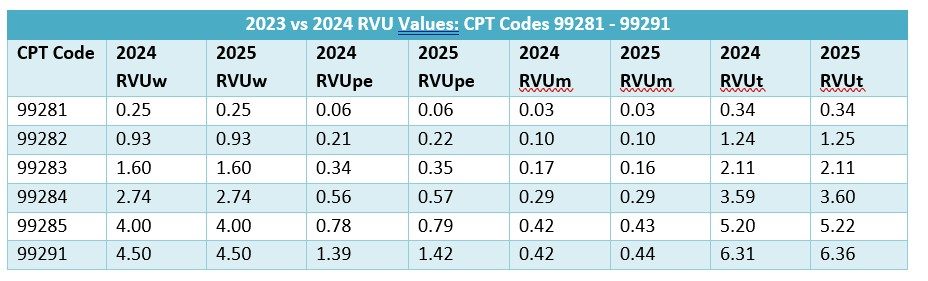
Relative Value Units for 2025
The 2025 emergency services Work RVU values are identical to the 2024 values.
Budget Neutrality Purgatory
The Medicare Physician Fee Schedule (MPFS) is the only major Medicare program subject to budget neutrality provisions. Drivers of Medicare fee schedules include:
- Part A: Hospitals – medical inflation
- Part B: Budget neutrality – MPFS
- Part C: Medicare Advantage costs – 8% increase in 2023
- Part D: Prescription drugs – variety of factors
Since 2020, the conversion factor has decreased by 10.37%. At best, budget neutrality provisions lock in flat MPFS rates in the future before inflation. The potential for continued CF reductions exists every time a new code is added or RVUs are adjusted to favor certain physicians. Nothing will change unless Congress addresses the MPFS funding structure. Although there are currently bills introduced in Congress to address this inequity, the passage of such legislation in the near future remains uncertain. A startling note of comparison is a study performed by the Kaiser Family Foundation that revealed commercial insurance premiums increasing by 400% over the past 30 years. The study is available here: https://www.kff.org/report-section/ehbs-2023-section-1-cost-of-health-insurance/
Practice Expense RVUs
Practice expense RVUs remain a small fraction of total RVUs for emergency services CPT codes, with work RVUs comprising the largest portion, by far. Historically, input for practice expense RVUs has been culled from surveys performed by the American Medical Association. The most recent survey was performed in spring 2024, the results of which are not yet released. Interestingly, the AMA survey included, for the first time, two pages of questions related to EMTALA-related bad debt. In the Final Rule, CMS states that they have hired the Rand Corporation to explore development of alternative methodologies to determine physician practice expenses. No action will occur in 2025, but possible changes in practice expense RVUs will occur in 2026.
CPT Versus HCPCS
Medicare has predominately used the AMA CPT® (Current Procedural Terminology) codes to determine the Medicare Physician Fee Schedule. Occasionally, Medicare has used HCPCS (Healthcare Common Procedure Coding System) codes to determine the fee schedule. The incoming administration has expressed antipathy regarding the AMA’s “monopoly” of the CPT codes and RVU valuations. There is therefore the possibility of major realignment of code set utilization and valuations, although such action would most likely take several years.