2024 Proposed CMS Rule for the Medicare Physician Fee Schedule
2024 Proposed CMS Rule for the Medicare Physician Fee Schedule
In July, CMS published the Proposed Rule for the 2024 Medicare physician fee schedule. Overall, BSA Healthcare estimates that emergency medicine will undergo a 1% to 3% decrease in payments in 2024 compared to 2023 payments.
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
Budget neutrality provisions in the Medicare Physician Fee Schedule mandate a reduction in the 2024 conversion factor. CMS estimates a 2024 conversion factor of $32.7476. Compared to the 2023 conversion factor of $33.8872, the 2023 conversion factor represents a 3.3% decrease. Like previous years when Congress passed one-time fixes to the SGR formula, Congress in 2022 passed a 2.5% increase in the conversion factor that mitigated a 3% reduction in the conversion factor in 2023. Half of that 2.5% increase – 1.25% – carries over to the 2024 conversion factor. The remaining 1.25% reduction in the conversion factor increases to a 3.36% reduction when CMS includes a budget neutrality 2.1% reduction caused by the initiation of a new HCPCS code – G2211 (add-on complexity for office visits) – that emergency medicine is not eligible to use. The final 2024 conversion factor is due to be published in November 2023. There is a possibility of late-year Congressional action to mitigate the CF decrease, including delay of G2211 implementation.
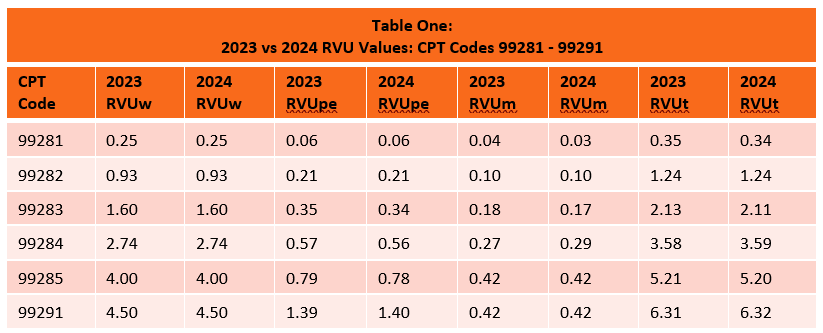
Relative Value Units for 2024
CMS has proposed minimal RVU changes for emergency service code practice expense and malpractice RVUs in 2024. Work RVUs remain unchanged for 2024. Overall, emergency service code RVUs are flat in the proposed rule.
Budget Neutrality Provisions Affecting the Conversion Factor
Because CMS is statutorily mandated to maintain budget neutrality when changes are made to the physician fee schedule, the 2021 RVU increases for office visit codes caused a reduction in the conversion factor for all CPT codes, including emergency services.
At the end of 2020, Congress mitigated the significant reduction in the 2021 conversion factor by adding a one-time increase of 3.75% to the conversion factor. At the end of 2021, Congress mitigated the significant reduction in the 2022 conversion factor by adding a one-time 3% increase to the conversion factor. At the end of 2022, Congress mitigated the significant reduction in the 2023 conversion factor by adding a 2.5% increase to the conversion factor in 2023 and 1.25% in 2024. The proposed initiation of the G2211 code in 2024 will cause another 2.1% reduction to the conversion factor. Pay-as-you-go budgetary 4% sequestration reductions are suspended through 2024, however the ongoing 2% sequestration remains in effect. In sum, emergency medicine is facing a potential 1-3% reduction in payments caused by the conversion factor decrease.
Medicare’s budget neutrality provision for Part B physician services stands in stark contrast to federal funding mechanisms for Part A (hospitals), Part C (Medicare Advantage), and Part D (prescription drugs). Funding for these other three Parts is based on inflationary or cost increases. Strikingly, commercial insurer Medicare Advantage Plans received an 8% funding increase for 2023 despite many of these plans being under federal fraud investigation for hundreds of millions of dollars of overpayments based on deceptive diagnostic coding. Only Congress can change Medicare funding formulas, so Congressional action is required to modify the Part B budget neutrality provision.
Budget Neutrality Purgatory
Since 2020, the conversion factor has decreased by 9.25% from 36.0893 to 32.7476. At best, budget neutrality provisions lock in flat MPFS rates in the future before inflation. The potential for continued CF reductions exists every time a new code is added or RVUs are adjusted to favor certain physicians. Nothing will change unless Congress addresses the MPFS funding structure.
One remote possibility for enhanced funding for emergency services exists in the form of EMTALA-related funding for physicians who provide safety net services. The Emergency Medicine Practice Institute is financially backing an effort to develop an effective EMTALA narrative. Success is by no means guaranteed. It will take years and will require Congressional action.
Shared Services
In the Proposed Rule, CMS again clarified that services provided by a physician and a non-physician practitioner in the same group should be billed by the provider that performs a substantive portion of the visit (more than 50%). To determine “substantive portion” CMS will rely upon time. Since time is not used in determination of emergency service E/M codes, last year CMS requested public comments on other methods for determination of what qualifies as the “substantive portion” for emergency services. In this year’s Proposed Rule, CMS again deferred the mandatory use of time for shared emergency services until 2025.