2024 Final CMS Rule for the Medicare Physician Fee Schedule: CMS-1784-F
2024 Proposed CMS Rule for the Medicare Physician Fee Schedule
In November, CMS published the final rule for the 2024 Medicare Physician Fee Schedule (MPFS).
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
Budget neutrality provisions in the MPFS mandate a reduction in the 2024 conversion factor. CMS assigned a 2024 conversion factor of $32.7442, which is approximately 3.37% lower than the 2023 conversion factor of $33.8872. A new code G2211 – add-on complexity to office visits – reduced the CF by 2.1% (budget neutrality) and expiration of half the 2.50% CF increase passed by Congress at end of 2023 caused a 1.25% reduction.
Potential Congressional action to mitigate the CF decrease is very uncertain. In prior years Congress has passed stopgap increases in the conversion factor as part of their end-of-year budget package. In 2023, Congress adjourned before passing a continuing budget resolution. Votes on two continuing resolutions are scheduled for the beginning of 2024. It is possible that Congress will still increase the 2024 conversion factor, although the Washington political environment makes this increase far from certain.
Sequestration
The 2022 end-of-year Congressional legislation contained two important provisions affecting physician reimbursement.
1. The continuation of the 2% sequestration cut.
2. The 2023 pay/go 4% sequestration cut was postponed until 2025.
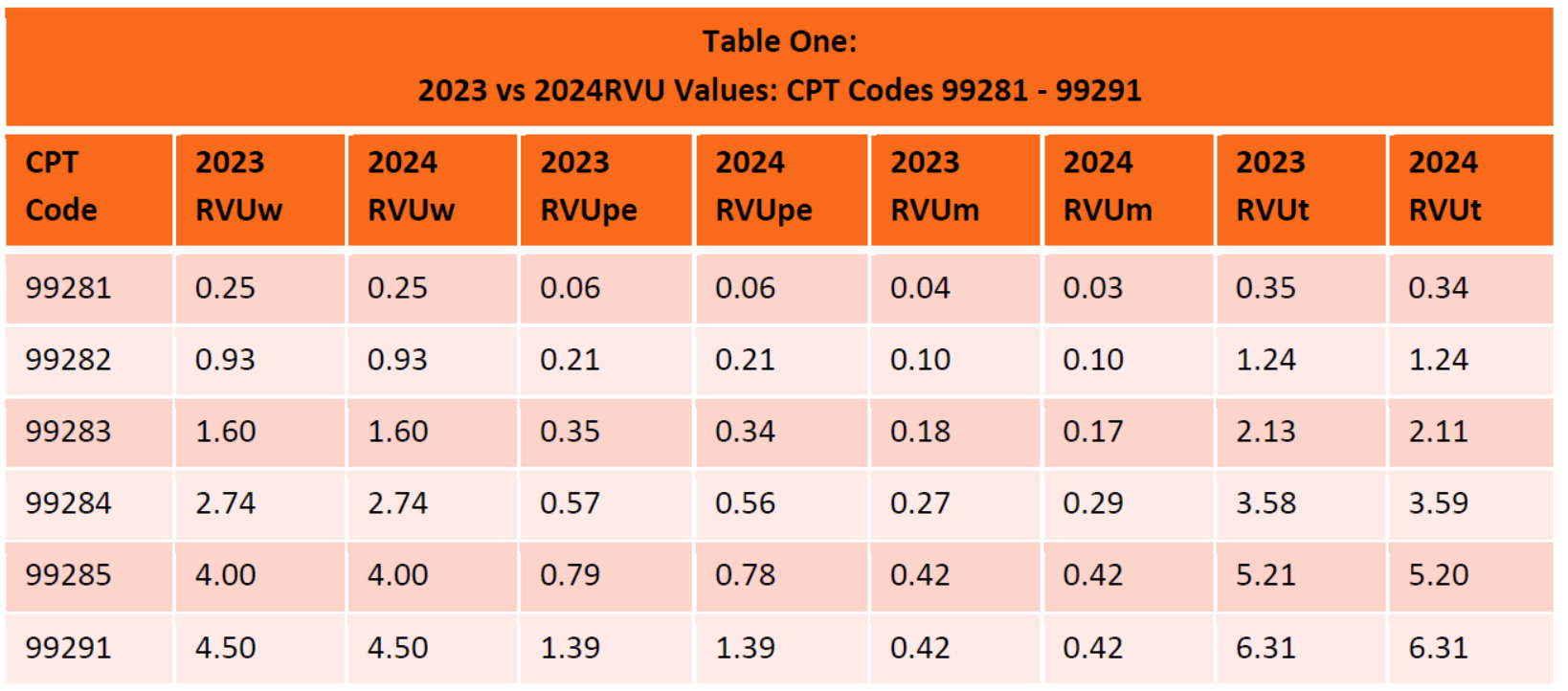
Relative Value Units for 2024
Emergency services RVUs are essentially unchanged from 2023 (see Table 1). In comparison to 2023, emergency service Work RVU values are identical.
Budget Neutrality Purgatory
The Medicare Physician Fee Schedule (MPFS) is the only major Medicare program subject to budget neutrality provisions. Drivers of Medicare fee schedules include:
• Part A: Hospitals – medical inflation
• Part B: Budget neutrality – MPFS
• Part C: Medicare Advantage – costs – 8% increase in 2023
• Part D: Prescription drugs – variety of factors
Since 2020, the conversion factor has decreased by 9.25% from 36.0893 to 32.7442. At best, budget neutrality provisions lock in flat MPFS rates in the future before inflation. The potential for continued CF reductions exists every time a new code is added or RVUs are adjusted to favor certain physicians. Nothing will change unless Congress addresses the MPFS funding structure. Although there are currently bills introduced in Congress to address this inequity, passage of such legislation remains unlikely in the near future.
One remote possibility for enhanced funding for emergency services exists in the form of EMTALA-related funding for physicians who provide safety net services. The Emergency Medicine Practice Institute is financially backing an effort to develop an effective EMTALA narrative. Success is by no means guaranteed. It will take years and will require Congressional action.
Shared Services
CMS continues to state that services provided by a physician and a non-physician practitioner in the same group should be billed by the provider that performs a substantive portion of the visit (more than 50%).
To determine “substantive portion” CMS will generally rely upon time. For services performed in a facility (such as emergency services), CMS will now rely either upon time or who performed the substantive portion of medical decision making for the involved CPT code.