2023 Proposed CMS Rule for the Medicare Physician Fee Schedule
2023 Proposed CMS Rule for the Medicare Physician Fee Schedule, and BSA Healthcare is working to ensure that our clients will be ready!
In July, CMS published the Proposed Rule for the 2023 Medicare physician fee schedule. Overall, BSA Healthcare estimates that emergency medicine will undergo a 1% to 10% decrease in payments in 2023 compared to 2022 payments.
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
Budget neutrality provisions in the Medicare Physician Fee Schedule mandate a reduction in the 2023 conversion factor. CMS estimates a 2023 conversion factor of $33.0775. Compared to the 2022 conversion factor of $34.6062, the 2023 conversion factor represents a 4.4% decrease. Like previous years when Congress passed one-time fixes to the SGR formula, Congress in 2021 passed a one-time 3% increase in the conversion factor that mitigated a 3.75% reduction in the conversion factor in 2022. To avoid all, or part, of the 2023 conversion factor reduction of 4.4% Congress will again need to pass end-of-year legislation to increase the conversion factor.
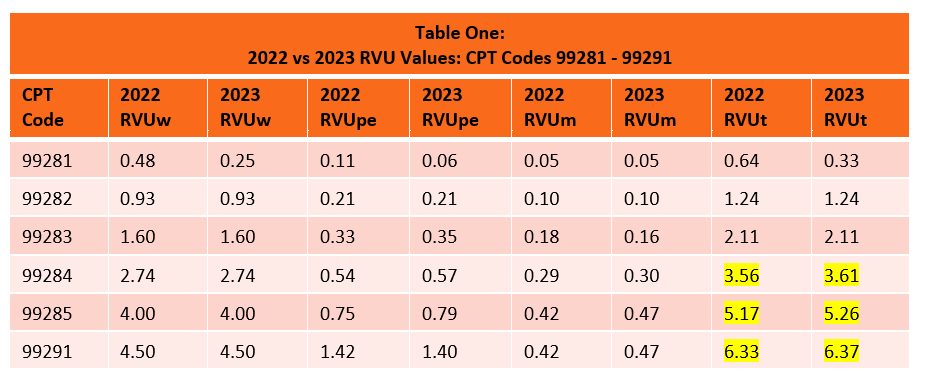
Relative Value Units for 2022
CMS has proposed minimal RVU changes for emergency service code practice expense and malpractice RVUs in 2023. Work RVUs remain unchanged for 2023 except for a decrease in E/M code 99281, which is rarely used. Significantly, CMS kept the RVUw for 99284 unchanged after the AMA RUC Committee had recommended a decrease to 2.60. Overall, emergency service code RVUs have increased by 1% in the proposed rule due to small RVU increases in practice expenses and malpractice. Of note, in past years small RVUpe and RVUm increases in the proposed rule have vanished in the final rule.
Budget Neutrality Provisions Affecting the Conversion Factor
Because CMS is statutorily mandated to maintain budget neutrality when changes are made to the physician fee schedule, the 2021 RVUw increases for office visit codes caused a reduction in the conversion factor for all CPT codes, including emergency services.
At the end of 2020, Congress mitigated the significant reduction in the 2021 conversion factor by adding a one-time 3.75% to the conversion factor. At the end of 2021, Congress mitigated the significant reduction in the 2022 conversion factor by adding a one-time 3% increase to the conversion factor. With the expiration of this one-time conversion factor increase, physicians are facing a 4.4% reduction in 2023 payments. Pay-as-you-go budgetary rules will add another 4% sequestration reduction in 2023, in addition to an ongoing 2% sequestration. In sum, emergency medicine is facing a potential 9.5% reduction in payments caused by 6% sequestration cuts and a 4.5% conversion factor decrease, with a minimal offset of a potential 1% increase in RVUs.
Medicare’s budget neutrality provision for Part B physician services stands in stark contrast to federal funding mechanisms for Part A (hospitals), Part C (Medicare Advantage), and Part D (prescription drugs). Funding for these other three Parts is based on inflationary or cost increases. Strikingly, commercial insurer Medicare Advantage plans received an 8% funding increase for 2023 despite many of these plans being under federal fraud investigation for hundreds of millions of dollars of overpayments based on deceptive diagnostic coding. Only Congress can change Medicare funding formulas, so Congressional action is required to modify the Part B budget neutrality provision.
BSA Healthcare Opinion: Emergency Medicine needs to engage in vigorous coalition advocacy efforts in order to suspend and permanently change the budget neutrality provision of the MPFS and to avoid sequestration fee reductions.
Shared Services
In the Proposed Rule, CMS again clarified that services provided by a physician and a non-physician practitioner in the same group should be billed by the provider that performs a substantive portion of the visit (more than 50%). To determine “substantive portion” CMS will rely upon time. Since time is not used in determination of emergency service E/M codes, last year CMS requested public comments on other methods for determination of what qualifies as the “substantive portion” for emergency services. In this year’s Proposed Rule, CMS deferred the use of time for shared emergency services until 2024, but further deferrals seem unlikely.