2023 Final CMS Rule for the Medicare Physician Fee Schedule: CMS-1770-F
2023 Final CMS Rule for the Medicare Physician Fee Schedule: CMS-1770-F
In November, CMS published the final rule for the 2023 Medicare Physician Fee Schedule (MPFS). Subsequent to release of the Final Rule, Congress passed a bill that affected 2023 Medicare physician payments. The bill’s impact on emergency medicine reimbursement is addressed in this issue.
The basic payment formula remains: (RVU work x GPCI work) + (RVU P.E. x GPCI P.E.) + (RVU M x GPCI M) = RVU TOTAL x Conversion Factor = Fee for each CPT® Code
Conversion Factor Updates
Budget neutrality provisions in the MPFS mandated a dramatic reduction in the 2023 conversion factor. CMS assigned a 2023 conversion factor of $33.0607, which is approximately 4.5% lower than the 2022 conversion factor of $34.6062. This 4.5% reduction, originally scheduled to go into effect in 2023, was mainly due to budget neutrality provisions of the MPFS. Congress passed Omnibus legislation at 2022 year-end that mitigated 2.5% of the reduction in the conversion factor for 2023. Combining the 4.5% CMS reduction in the conversion factor and the 2.5% Congressional increase in physician fees results in an approximate 2.0% reduction in the conversion factor in 2023.
Sequestration
Prior to 2022 end-of-year Congressional action, two sequestration cuts to Medicare payments were also scheduled to go into effect on January 1, 2023. These included the long-standing 2% sequestration cut, and a 4% sequestration cut secondary to pay/go regulations related to the 2021 COVID Relief Package.
The 2022 end-of-year legislation contained two important provisions affecting physician reimbursement.
- The continuation of the 2% sequestration cut.
- The 2023 pay/go 4% sequestration cut is being postponed until 2025.
In summation, the potential 10.5% reduction in the 2023 MPFS was decreased by Congress to a 4.5% reduction.
Relative Value Units for 2023
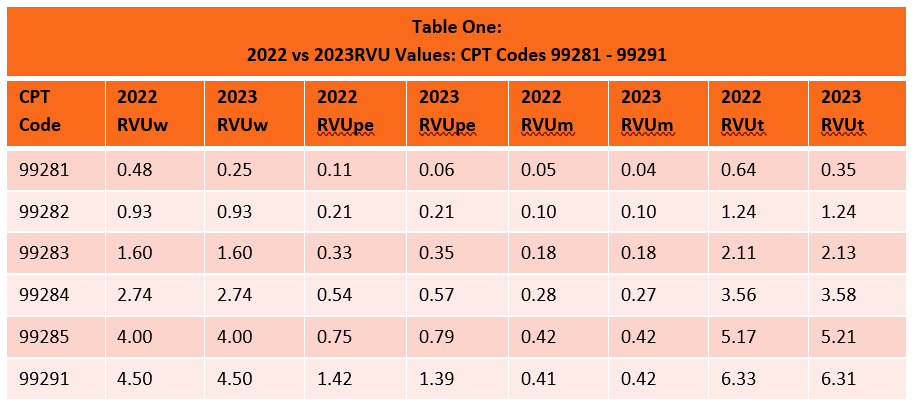
Emergency services RVUs are essentially unchanged from 2022 (see Table 1). 2023 practice Expense RVUs reflect minor changes compared to 2022, as did malpractice RVUs. In comparison to 2022, emergency service Work RVU values are identical, with the exception of the rarely used 99281 code. Importantly, CMS rejected an AMA-RUC recommendation that would have lowered the RVUwork for 99284 from 2.74 to 2.60.
Revisiting the 2021 CMS Redistribution Process
In 2021, CMS finalized groundbreaking payment policy changes that resulted in significant redistribution of Medicare physician payments to primary care providers in office-based settings via implementation of significant increases in Work RVUs for office visit CPT codes based upon a revaluation exercise performed by the AMA RUC. In addition, CMS recommended that two additional codes be allowed for use by primary care providers. Congress postponed the use of one of these codes – G2211 – for three years.
Via the budget neutrality provisions of the Medicare Physician Fee Schedule, increases in office visit payments will come at the expense of providers who derive payments from sites of service outside of an office. Emergency services fall into this latter category. Payments for evaluation and management services currently compose 40% of Medicare physician payments, with office visits accounting for half of that amount. By increasing office visit payments across the board, budget neutrality requires a reduction in Medicare payments for all other CPT codes. The mechanism that CMS uses in order to maintain budget neutrality is a reduction in the conversion factor. Fortunately, for emergency service CPT codes, linkage to office visit work RVUs increased the work RVUs for emergency services and mitigated a significant portion of the conversion factor reduction.
Shared Services
CMS clarified that services provided by a physician and a non-physician practitioner in the same group should be billed by the provider that performs a substantive portion of the visit (more than 50%). To determine “substantive portion” CMS deferred relying solely upon time until 2024 for emergency services. For 2023, substantive portion may be calculated either by using time or history/exam/MDM.
Medical Economic Index (MEI) Rebasing
Medicare is in the process of rebasing their medical economic index, which accounts for inflation. The MEI plays an important role in determination of GPCI values and the RVU for practice expense. Changes to RVUpe are deferred until 2024. ACEP is actively involved in this process. There is a danger of a budget neutrality decrease in emergency services fees without the inclusion of bad debt, standby expenses, and undercompensated care in the calculation of the MEI for emergency medicine.
Critical Care
CMS finalized changes to the threshold for reporting CPT 99292. Despite advocacy from emergency medicine, the threshold increased from 75 to 104 minutes.
Telehealth
CMS added the five emergency services E&M codes and the critical care codes to the approved telehealth list until 12/31/23.
2023 Documentation Guidelines
Implemented on January 1st, 2023, the new 2023 E/M Documentation Guidelines seek to provide continuity across all the E/M sections allowing for revisions implemented in the E/M office visit section in 2021 to extend to all other E/M sections – including emergency medicine and hospitalist E/M codes – with revisions to the Levels of Medical Decision Making (MDM) table and retirement of some HM codes. A proactive and thorough approach will ensure compliance and keep the revenue flowing following implementation of the new DGs in your organization.
In order to prepare your staff, BSA Healthcare has created the following:
A web-based Emergency Medicine Provider Documentation Webinar Library
In order to assist organizations in preparation of coder and provider staff, BSA Healthcare is offering the following:
- A web-based Emergency Medicine Coder Training Webinar Library – Worth 4 Core A CEUs or CEDC credits to your certified coders!
- A web-based Emergency Medicine Provider Training Webinar Library.
- A web-based Hospitalist Medicine Provider Documentation and Coder Training Webinar Library.
- Newly revised Emergency Medicine and Hospitalist Coder Desktop Reference Tools.
- Interested in virtual, live training of your ED or HM coding staff? We offer that too!
We have also updated our proprietary audit software for the new DGs and are offering 100-record focused audits of charts coded using the new DGs. External focused audits should be done almost immediately following implementation in order to:
- Identify risks and quickly evaluate if a larger audit should be performed.
- Safeguard your organization’s revenue.
- Ensure compliance with new regulatory requirements.
- Provide resolution over new DG coding controversies that are being debated within your organization.
- Identify coding policies that may need adjustment and code choice patterns that could result in compliance violations.
- Isolate individual providers and coders who may require additional documentation and/or coder education.
For additional information, deliverables, or fee information for any of our new 2023 DG products or service offerings, please call 888.568.4993, or email jjones@bsanda.com.